|
DEPARTMENT RESULTS |
|
|
| |
|
Goal: All children get a
healthy start in life |
|
Why is this goal important?
Each year approximately 70,000 babies are born in Minnesota representing
a new cohort of children. Each new cohort in all geographic areas, racial
and ethnic groups and socioeconomic strata should have access to preventive
services, screening and early interventions that will help them lead
healthy, productive lives. Reducing infant mortality rates, ensuring proper
screenings, receiving on time immunizations and providing earlier
interventions improve the lives of all Minnesotans by ensuring an equal
opportunity to enjoy good health.
A healthy
birth depends on many factors: the mother’s health before pregnancy, family
and social support, access to health care, quality and content of prenatal
care, nutrition and appropriate weight gain during pregnancy, the absence of
violence and injury, and abstention from substances such as tobacco, alcohol
and drugs. Although Minnesota’s overall infant mortality rate is low, some
populations such as American Indians and African Americans, are higher than
the majority white population. While gaps in infant mortality still exist
among American Indians and populations of color in Minnesota, the data below
shows that the gap has narrowed.
Immunizations protect
children from diseases that used to take their lives or permanently damage
them. It is important that children receive all recommended immunizations by
the time they turn two years old, since it is during this time period that
they are the most vulnerable to severe complications of diseases such as
whooping cough, hepatitis B, and measles. Children may not have received all
recommended vaccines because their parents do not understand the importance
of vaccination, have competing priorities or do not know when the next shot
is due.
Lead poisoning is the most common pediatric
environmental health problem for young children. It can damage a child's
central nervous system, kidney and reproductive organs and cause learning
and behavioral problems. Children are exposed to lead in the air, in food,
in drinking water, from the glaze on pottery dishes and, most often, from
lead-based paint, by eating lead-laced dust or paint chips. |
| |
|
What is
MDH doing to achieve this goal?
·
Reduce infant mortality rates in every racial and ethnic
population.
In 2001 the MDH launched a
major initiative to address health disparities in several key areas,
including infant morta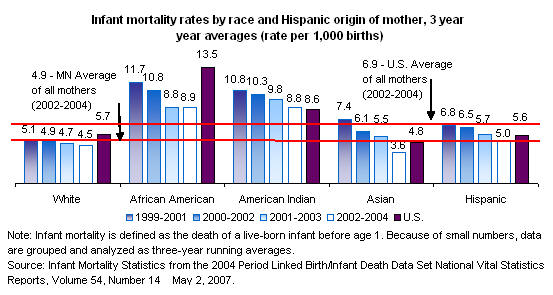 lity. In the last
five years, over 50 community-based
organizations have received grants to develop innovative and effective
methods to reduce health disparities in American Indians and populations of
color. The MDH is providing technical assistance and support to help these
organizations reach out to their communities and find strategies that work. lity. In the last
five years, over 50 community-based
organizations have received grants to develop innovative and effective
methods to reduce health disparities in American Indians and populations of
color. The MDH is providing technical assistance and support to help these
organizations reach out to their communities and find strategies that work.
·
Improve on-time childhood immunization rates.
In addition to measuring overall imm unization rates, the MDH distributes
publicly purchased vaccines for children whose families are unable to afford
vaccines, communicates with schools and
health care providers on the school immunization law, works with public
health partners to develop immunization policies, maintains the Minnesota
Immunization Information Connection (a statewide immunization registry), and
provides information and education about vaccine-preventable diseases to
public health professionals and the public in printed pieces and on the Web. unization rates, the MDH distributes
publicly purchased vaccines for children whose families are unable to afford
vaccines, communicates with schools and
health care providers on the school immunization law, works with public
health partners to develop immunization policies, maintains the Minnesota
Immunization Information Connection (a statewide immunization registry), and
provides information and education about vaccine-preventable diseases to
public health professionals and the public in printed pieces and on the Web.
·
Reduce childhood exposure to lead. With the leadership of MDH, the
State of Minnesota continues to implement the "2010 Childhood Lead Poisoning
Elimination Plan." This comprehensive plan has a goal of creating a
lead-safe Minnesota where no child would have elevated blood lead levels by
the year 2010. It recommends using a collaborative, housing-based approach
to promote primary prevention of lead exposure while still incorporating
ongoing state and local programs that
are based on secondary prevention models. The threshold for environmental
intervention was recently lowered to a single venous blood lead test above
15 ug/dl (see graph for historical trend). The MDH also continues to promote
state guidelines on screening, case management, and clinical treatment of
children and pregnant women exposed to lead and conducts and oversees
inspections, assessments, and lead hazard abatements to help safely remove
lead from the environment.
 |
|
How is
the MDH’s progress?
The state’s target for 2010 is to reduce
the health disparities between rates for populations of color and rates for
whites. It will take time before a complex measure like infant mortality
will reflect the actions MDH is taking today. However, there has been a
slight decrease in all populations and there is a definite increase in
awareness of the issues and a growing commitment among many communities to
make a difference for tomorrow. Minnesota's overall infant mortality rate dropped
from 5.5 per thousand live births in 2000-2002 to 4.9 deaths per thousand
live births in 2002-2004. During these two comparison periods the rate
dropped lower for whites (from 4.9 to 4.5), for African Americans (from 10.8
to 8.9), for American Indians (from 10.3 to 8.8), for Asians (from 6.1 to
3.6) and for Hispanics (from 6.5 to 5.0).
Our target for immunization rates is that at least 90 percent of all infants
in all geographic areas, racial and ethnic groups, and socio-economic strata
will receive, within two months of the recommended age, age-appropriate
immunization against including diphtheria, tetanus, pertussis, polio,
measles, mumps, rubella, Haemophilus influenzae type B disease, hepatitis B,
pneumococcal disease, and varicella.
National lead poisoning rates have declined dramatically over the past 25
years and have maintained a gradual decline in recent years. In general,
Minnesota rates of lead exposure are generally slightly lower than the
national average. As screening becomes more efficient and targets high-risk
populations, the total number of elevated cases may actually increase,
although the rates of cases compared to total population will continue to
decline.
|
|
Learn
more about:
 Infant mortality
Infant mortality
Child immunization
Lead |
| |
|
Goal:
Everyone living healthy from adolescence into old age |
|
Why is
this goal important?
 Healthy
communities and preventive practices are key to good health. Healthier
people lead to a healthy society. Minnesotans need to understand the
importance of prevention as the best way to maintain good health. Tobacco
use is the leading cause of preventable death and disease in Minnesota.
Smoking causes heart disease, cancer, chronic lung disease, and other
diseases. Smokeless tobacco is associated with cancer of the gum, mouth,
pharynx, larynx and esophagus. Cigar smoking can cause oral, esophageal,
laryngeal and lung cancers. Smoking costs Minnesota approximately $2.64
billion in health-related economic costs each year. About one in five
Minnesota adults smoke cigarettes. Most adult smokers began their habit as
adolescents or earlier. The earlier one starts smoking, and the longer one
continues, determines the severity of tobacco’s health impact on the
individual. In addition, teens that smoke are also more likely to try other
substances or to get involved in other unhealthy activities. Healthy
communities and preventive practices are key to good health. Healthier
people lead to a healthy society. Minnesotans need to understand the
importance of prevention as the best way to maintain good health. Tobacco
use is the leading cause of preventable death and disease in Minnesota.
Smoking causes heart disease, cancer, chronic lung disease, and other
diseases. Smokeless tobacco is associated with cancer of the gum, mouth,
pharynx, larynx and esophagus. Cigar smoking can cause oral, esophageal,
laryngeal and lung cancers. Smoking costs Minnesota approximately $2.64
billion in health-related economic costs each year. About one in five
Minnesota adults smoke cigarettes. Most adult smokers began their habit as
adolescents or earlier. The earlier one starts smoking, and the longer one
continues, determines the severity of tobacco’s health impact on the
individual. In addition, teens that smoke are also more likely to try other
substances or to get involved in other unhealthy activities.
Early detection of cancer vastly improves an individual’s chance of
survival. The U.S. Preventive Services Task Force, under the Department of
Health and Human Services, recommends routine mammograms every 1-2 years for
women 40 years of age and older, and routine cervical cancer screening for
all women who are or have been sexually active and who have a cervix. The
current recommendation is to begin Pap testing within 3 years of the onset
of sexual activity or age 21 (whichever comes first) and screening at least
every three years. Screening is not recommended for women older than age 65
who have had adequate recent screening with normal pap tests and who are not
otherwise at high risk.
Regular physical activity reduces long-term risks to health, such as
overweight and obesity, heart disease and stroke, arthritis, diabetes,
osteoporosis, high blood pressure, and cancer. Unfortunately, for many
reasons, the number of adults who do not get regular physical activity has
been steadily going up. Physical inactivity creates a huge economic burden
on the state: an estimated $495 million was spent during 2000 to treat
diseases and conditions
that could be avoided if all Minnesotans were physically active.
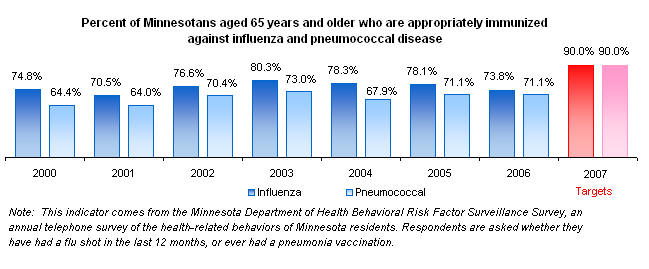
Although influenza and pneumonia cause disease in all age groups, they
are the fifth leading cause of death among
Americans age 65 and older. Vaccination reduces
the risk of serious
complications that can lead to hospitalizations
and death.
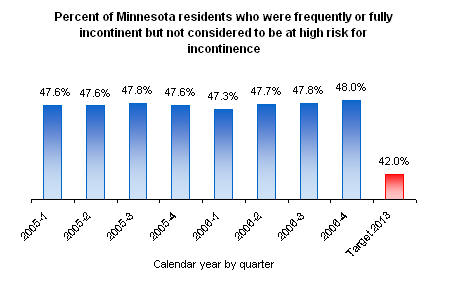
One identified quality of life and health problem for nursing home residents
is high rates of incontinence in residents who are not considered at high
risk for incontinence. Incontinence in many cases is reflective of the
quality of care provided. This area continues to fall within the top 10
problems identified in nursing home surveys. As an example, if low risk
residents are not being offered proper assistance to ensure reasonable and
timely assistance in toileting, it can be a signal of the culture, quality
of care, and approaches being implemented within the facility.
|
|
What is MDH doing to achieve this goal?
·
Reduce the percentage of youth who use tobacco. The MDH is using a
community-driven, evidence-based approach to reduce tobacco use among young
people. The approach includes strategies such as: helping communities work
on policy changes to reduce exposure to second-hand smoke; implementing
comprehensive school-based tobacco prevention programs; and reducing the
number of businesses that sell tobacco to minors.
· Increase the percent of women who receive
regular mammograms and pap smears to check for breast and cervical cancer.
The MDH coordinates and funds free/low cost cancer
screening services for
women who are uninsured or underinsured, including women identified as
needing follow-up to screening services. The MDH partners with the Minnesota
Department of Human Services, city and county public health agencies and
health providers as they develop strategies to find and assist women with
breast or cervical cancer. The MDH also educates the public about the
importance of screening and works to raise awareness of breast and cervical
cancer screening among health professionals. services for
women who are uninsured or underinsured, including women identified as
needing follow-up to screening services. The MDH partners with the Minnesota
Department of Human Services, city and county public health agencies and
health providers as they develop strategies to find and assist women with
breast or cervical cancer. The MDH also educates the public about the
importance of screening and works to raise awareness of breast and cervical
cancer screening among health professionals. |
|
·
Increase the percentage of adults who exercise
on a regular basis. The MDH has drawn attention to this issue by
providing information on the health care costs associated with a lack of
physical activity. A more comprehensive approach, however, is needed to help
Minnesotans of all ages become physically active. We need to address the
issues in our physical environments that keep adults as well as children
from regular walking, biking, or engaging in physically active recreation.
Opportunities for physical activity are needed for people in worksites,
schools and communities. Communication campaigns are needed to help people
understand the importance of physical activity to their health and to learn
how to incorporate more activity in their daily life.
·
Increase the percentage of older adults who receive immunizations.
The MDH provides guidance, support, and education to local public health
agencies and providers of immunizations in Minnesota, including:
| |

·
Establishing a yearly flu plan that provides an overview of
influenza vaccination issues for the coming season.
·Sending
two large mailings to health care providers and long term care
facilities and others including yearly flu plan, new physician pocket guide, vaccine storage and handling
information, and vaccine administration information.
·
Establishing a "Mark of Excellence" program for non-traditional
vaccine providers to provide specialized training in vaccine
handling and dispensing.
·
Putting our materials on the Internet, including listings of
non-traditional clinic sites via the "Find-A-Flu Clinic" page,
www.mdhflu.com
·Assisting
persons who call the MDH to locate flu clinics in their area.
 |
·
MDH's goal is to remain below the current national average of 48% of low
risk residents that are incontinent and to reduce to 42% over the next five
years. Maintain the quality of life for our elderly and most vulnerable
population living in nursing homes in regards to urinary incontinence. The
Centers for Medicare & Medicaid Services (CMS) through the use of the
Minimum Data Set (MDS) has a MDS Quality Measure/Quality Indicator for
Elimination/Incontinence. The MDS instrument is data submitted by each
nursing home to MDH based on the nursing home's assessment of the resident's
functional and behavioral capacity, health conditions, and medical
diagnosis. Minnesota has almost 18,000 nursing home residents identified as
low risk for incontinence. MDS data has identified approximately 48% or
approximately 8,000 of those residents as having frequent or persistent
problems with incontinence.
The MDS
quality indicator process is a practical means of helping facility staff to
gather and analyze information to improve a resident’s quality of care and
quality of life. The MDS incorporates all members of the interdisciplinary
team in a proactive process. MDH will continue to work with the quality
improvement organization, nursing home providers, consumers and families to
improve resident quality of care and quality of life to ensure the number of
residents impacted does not surpass the national average.
*Note: Starting in SFY’04, new federal
protocols were introduced emphasizing the prevention of urinary incontinence
and improving assessment of resident care needs by nursing home staff.
|
|
How is the MDH’s progress?
Tobacco use by
Minnesota’s youth continues to decline dramatically, according to the
Minnesota Youth Tobacco Study. Smoking has dropped by 43 percent among
middle-school students and 31 percent among high-school students between
2000 and 2005.
The most recent data indicates that the percentage of women screened for
breast and cervical cancer in Minnesota is somewhat higher than the national
median. The breast cancer mortality rate has been decreasing significantly
and steadily since the early 1990's in Minnesota and nationally.
Physical inactivity is a complex issue, with many significant barriers to
change. In addition, older adults are least likely to achieve the
recommended minimums for physical activity, so as the state’s population
ages this issue will become even more challenging.
The most recent data show a slight upturn in immunization rates for older
adults. To raise these rates, more messages need to be delivered about the
importance of older adult immunizations and where to go for shots. More
effort also needs to be targeted at populations of color and Native American
communities.
CMS data shows Minnesota is currently near the national average and is not
performing as well as other states in our region when preventing conditions
of resident incontinence. The average number of residents with urinary
incontinence across CMS-Region 5 is approximately 45.2% with Illinois having
the lowest average at 40.6% and Ohio with the highest number of residents at
49.6%. Nationally, the number of nursing home residents with urinary
incontinence has risen from 47.2% in the first quarter of 2005, to
48% in the last quarter of 2006. Minnesota's average is 48% in the 4th
quarter of 2006. Better performance in nursing home incontinence can affect
the quality of life and health of thousands of nursing home residents.
|
|
Learn
more about:
Adult immunization
Youth tobacco use prevention
Community strategies and resources to promote
physical activities |
| |
|
Goal: Minnesota is a healthy
place to live |
|
Why is
this goal important?
 Access
to clean water and food and early intervention of emerging health threats
leads to a healthier population and a healthier society. Arsenic occurs
naturally in the environment and can work its way into groundwater.
Long-term exposure to elevated levels of arsenic is associated with an
increased risk of some cancers and problems with the circulatory and nervous
systems. Long-term exposure to elevated levels of radium is associated with
an increased risk of cancer. Research, and experience, has shown that
restaurants and other food establishments that have professionally trained
personnel are performing better at following safe food handling practices. Safe
food handling prevents food borne disease. Through a public-private
partnership between the Minnesota Public Health Laboratory and laboratories
statewide, Minnesota will be better able to detect and respond rapidly to a
suspected terrorism event involving biological agents. Access
to clean water and food and early intervention of emerging health threats
leads to a healthier population and a healthier society. Arsenic occurs
naturally in the environment and can work its way into groundwater.
Long-term exposure to elevated levels of arsenic is associated with an
increased risk of some cancers and problems with the circulatory and nervous
systems. Long-term exposure to elevated levels of radium is associated with
an increased risk of cancer. Research, and experience, has shown that
restaurants and other food establishments that have professionally trained
personnel are performing better at following safe food handling practices. Safe
food handling prevents food borne disease. Through a public-private
partnership between the Minnesota Public Health Laboratory and laboratories
statewide, Minnesota will be better able to detect and respond rapidly to a
suspected terrorism event involving biological agents.
|
|
 What
is MDH doing to achieve this goal? What
is MDH doing to achieve this goal?
·
Reduce exposure to arsenic and radium in the water supply.
Minnesota's public water systems must meet new Safe Drinking Water Act
(SWDA) standards for arsenic and radium. Most drinking water systems have taken a
proactive approach in meeting these standards before regulatory deadlines
occurred. Early compliance with the new standards has reduced the amount of
public exposure to these contaminants, prevented SDWA violations and related
enforcement activities, and provided a better opportunity for systems to
obtain low interest loans and grants.
The MDH monitors Minnesota's 962
community public drinking water systems serving 75% of our residential
population and 6383 non-community public drinking water systems serving
Minnesota citizens and visitors. The MDH originally identified 90 systems
with results exceeding the arsenic standard, and 60 systems with results
exceeding the radium standard.
Compliance with these standards requires
expensive and time-consuming infrastructure improvements, making it
difficult for many systems to come into compliance before the regulatory
deadlines. Despite these difficulties, the number of systems with arsenic
exceedances have been reduced to less than 20, and systems with radium
exceedances have been reduced to less than 20.
·
Increase the percent of eating places that have trained and certified
food managers, to ensure safe food handling practices. The MDH is taking
a very proactive approach to regulation in food establishments, working with
owners and managers to prevent problems before they occur. Previous
approaches to food safety in restaurants depended more heavily upon
inspections and corrective actions. The requirement that food establishments
have a certified food manager began in 2001, opening the door for the MDH to
provide preventive technical assistance to food establishments.
·
Increase the percent of Minnesota laboratories with the ability to
recognize possible agents of bioterrorism. The State Public Health
Laboratory provides hands-on laboratory training to assure that Minnesota
laboratories have the ability to recognize possible agents of bioterrorism.
Possible agents must be sent to the State Public Health Laboratory for
further analysis and specific identification. |
|
How is
the MDH’s progress?
Based on MDH’s monitoring program, 70 systems have made modifications to
their water system to reduce their arsenic to acceptable levels, and more
than 40 systems have made modifications to reduce radium levels. Our staff
worked with these systems to determine options for reducing the levels of
contamination in the water. We have also conducted seminars to disseminate
information about each contaminant. Minnesota is ahead of most states in
meeting these goals because of our proactive drinking water monitoring and
technical assistance programs. modifications to reduce radium levels. Our staff
worked with these systems to determine options for reducing the levels of
contamination in the water. We have also conducted seminars to disseminate
information about each contaminant. Minnesota is ahead of most states in
meeting these goals because of our proactive drinking water monitoring and
technical assistance programs.
The
Certified Food Manager (CFM) program began in 2000. This program is an
important component to ensuring that food is served safely in food
establishments throughout Minnesota. Managers and employees become certified
food managers after attending an educational course about how to control
risk factors that cause foodborne illness and passing an exam. A certified
food manager works in partnership with the Minnesota Department of Health,
the Minnesota Department of Agriculture, local health agencies, and
establishment owners to prevent problems before they occur in food and
lodging establishments.
The food service industry has a constantly changing
workforce. Over the past seven years, the CFM program has issued 58,244
certificates. As of June 2007, there are 25,556 current certified food
managers in Minnesota.
In 2006, 6,998 food inspections conducted by
the Minnesota Department of Health required a certified food manager. Of
those inspections, 15% or 1,039 establishments' owners were told to employ a
certified food manager; 85% of the establishments inspected in 2006 had a
certified food manager.
The MDH Public Health Lab has worked with
laboratories across the state to achieve their goal of increasing capacity
for recognizing possible agents of bioterrorism. In 2005, all licensed
laboratories had the ability to recognize Anthrax and 85% could detect
Brucella, achieving the department’s goal.
|
|
Learn
more about:
Water supply and exposure to arsenic and radium |
|
Some images © 2005 www.clipart.com
|
|
Last update on
06/28/2007 |
|